3rd Ventricular Colloid Cyst
Transsulcal transventricular excision of a 3rd ventricle roof colloid cyst
Dr Mrudul Bhatjiwale
6/4/20254 min read
Preoperative Imaging
T1 images and T2 images are crucial to identify the likely consistency of cyst contents and the position of surrounding veins, namely the thalamostriate veins, the septal veins and their confluence to form the internal cerebral veins. Colloid cysts rarely enhance on contrast imaging.
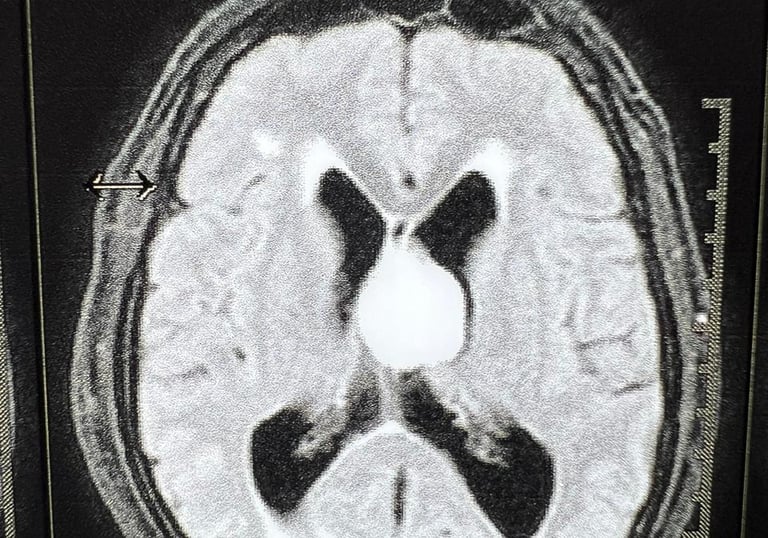
T2 FLAIR AXIAL
FLAIR hyper intense cystic lesion predominantly occupying the foramen of Monro. The ventricles are dilated with periventricular lucency suggesting increased intraventricular pressures.

T1 CORONAL
T1 hyper intensity is often suggestive of thick mucoid contents. Here the fornices are noted displaced towards the right, with the cyst predominantly in the left lateral ventricle.
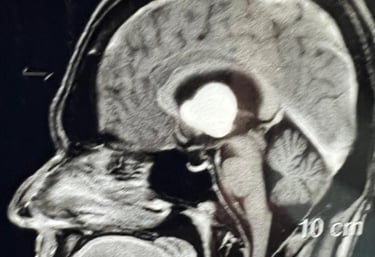
Shows multilobulated appliance of the cyst with extension upto the floor of the 3rd ventricle. It is crucial to study the extent of the cyst to plan the trajectories.
T1 SAGITTAL



Positioning and Exposure
In view of dilated ventricles and a large cyst extending into the left frontal horn predominantly, with displacement of the fornices to the right, a left transsulcal trans ventricular approach was planned.
PATIENT POSITION & INCISION
Supine, head neutral, on Mayfield head clamp. Keeping the head straight maintains midline orientation. A curvilinear incision was marked extending from the tragus to across the midline, behind the hairline.


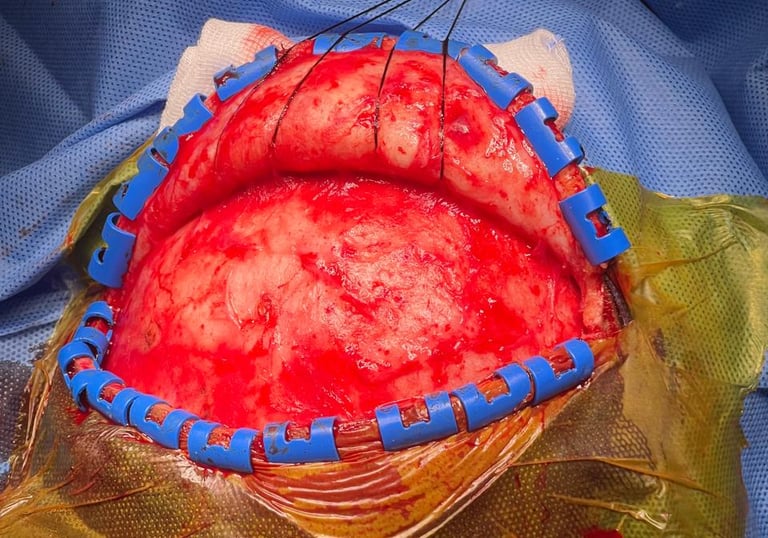
SCALP DISSECTION
Scalp flap retracted with silk sutures in layers. Pericranial flap reflected as a separate layer. The temporalis muscle need not be reflected as infra-Sylvain exposure is not required. Interfascial or subfascial dissection is carried out to preserve the frontalis branch of the Facial nerve.
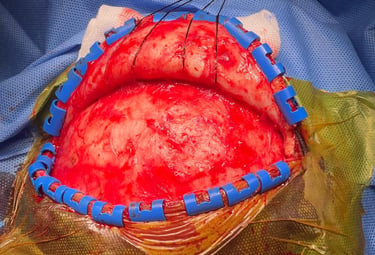
A left frontal craniotomy is performed using a single burr hole near the midline or two burr holes as required. The dura is opened based on the superior sagittal sinus exposing the middle and inferior frontal gyri and the inferior frontal sulcus.
CRANIOTOMY & DURAL OPENING


Surgical Nuances
In cases of large or giant colloid cysts, it is crucial to drain the cyst before attempting to excise the capsule to avoid unnecessary brain retraction and forniceal injury.
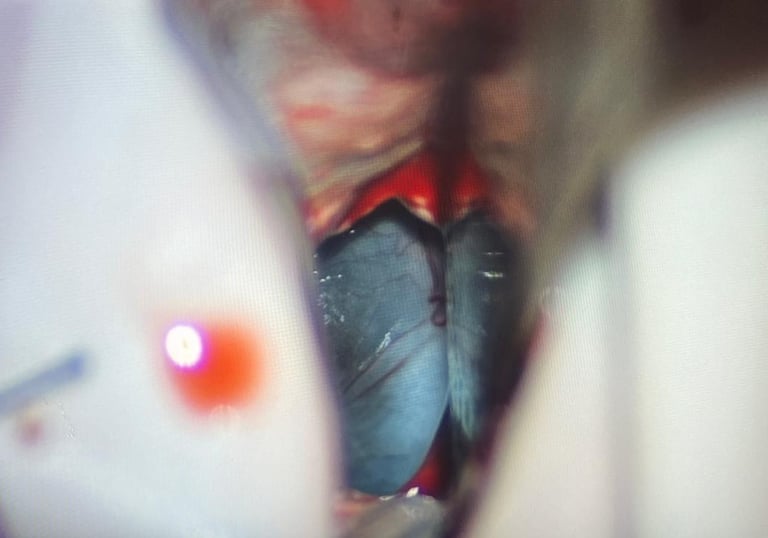
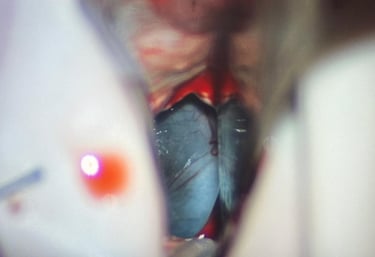
CYST EXPOSURE
On dissecting the inferior frontal sulcus, the sulcal trajectory is continued in the underlying white matter to reach the ventricle. A gush of CSF confirms ventricular entry. Exposure is widened and two Leyla retractors are introduced (or a tubular retractor) over rubber patties, to prevent parenchymal injury. Colloid cysts are encountered, face on, if the trajectory is right.
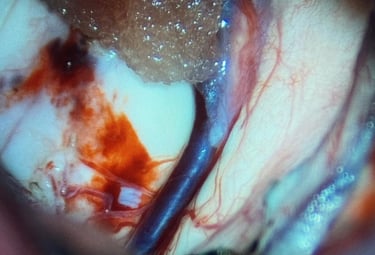
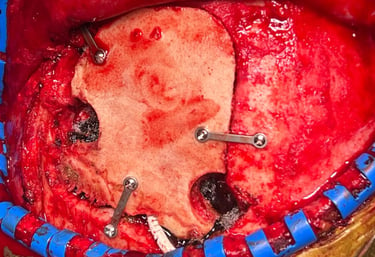
CYST EXCISION
Cyst is initially decompressed and its capsule is meticulously dissected off the fornices and surrounding veins. An arachnoid layer often helps guides dissection. The image shows the floor of the lateral ventricle (left), the thalamostriate vein (centre) and the septum pellucidum (right) after complete cyst wall excision. Care must be taken at the roof of the third ventricle where the cyst originates and sharp dissection under vision is essential. Blunt dissection in blind spots may be disastrous.
After ensuring free flow of CSF and wide opening of the foramen of Munroe and third ventricle, an EVD is placed in the third ventricle to drain any ooze that may occur. The EVD is removed after 24 hours if the CSF is clear.
EVD PLACEMENT



Closure and Postoperative Imaging
In cases of large or giant colloid cysts, it is crucial to drain the cyst before attempting to excise the capsule to avoid unnecessary brain retraction and forniceal injury.
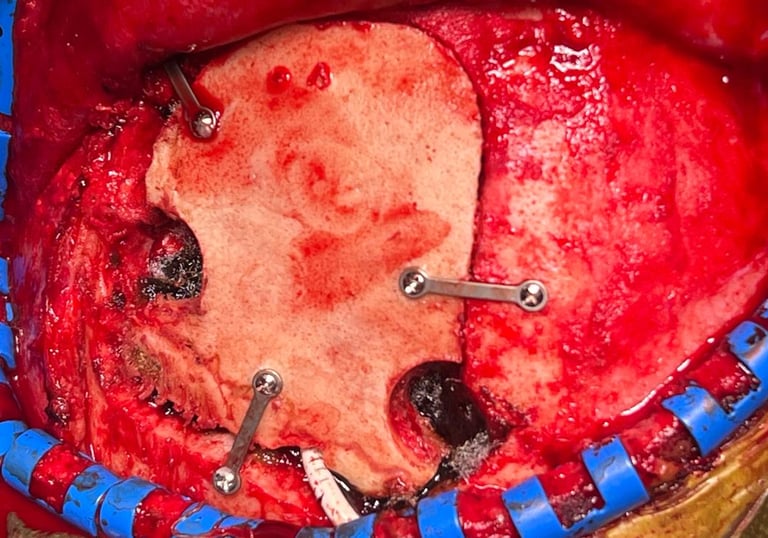
DURAL AND BONE CLOSURE
The dura is closed primarily over the external ventricular drain. It is brought out from one of the burr holes or from a gap in the bone after ensuring no kinks are present. Bone is fixed with a minimum of 3 manipulates and screws.
Patient was extubated on table.
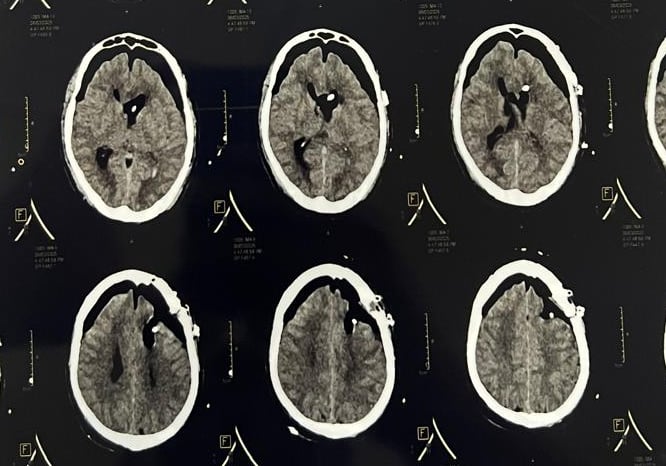
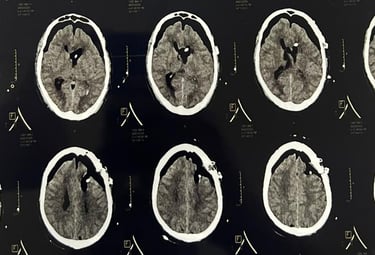
POD-0 CT BRAIN AXIAL
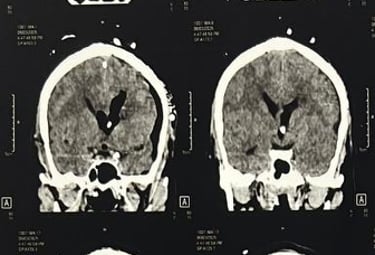
Complete resolution of the hydrocephalus with a lax brain with no intraventricular haemorrhage or tract bleed.
The external ventricular drain in situ in the third ventricle with complete excision of the cyst and communication of both the lateral as well as the third ventricle.
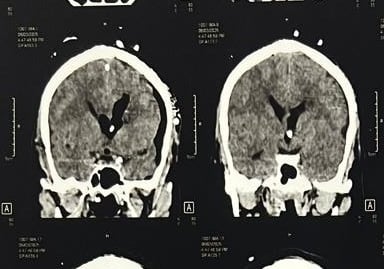
POD-0 CT BRAIN CORONAL
POST OP DAY 1
Recent, and remote memory both intact.
Power normal in all groups.
No neurodeficits with complete resolution of preoperative headache and confusion.
(Picture published with permission)




Contact Us
We would love to hear from you!
For appointments kindly use the Consult portal.
Email: drmrudulbhatjiwale@gmail.com
Phone: +91-8421190149
© Mrudul Bhatjiwale 2025. All rights reserved.