Dorsal Schwannoma Excision
Gratifying tumours with rewarding results if done meticulously. A step by step guide.
Dr Mrudul M Bhatjiwale
6/5/20253 min read
Preoperative Imaging
A dorsal schwannoma is a well circumscribed tumour which usually arises from one of the dorsal sensory roots. A good arachnoid plane from the spinal cord and a dorsal location makes excision relatively simple and gratifying, with the tumour practically presenting itself for excision.
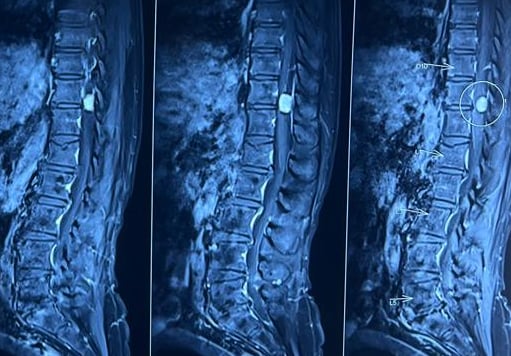
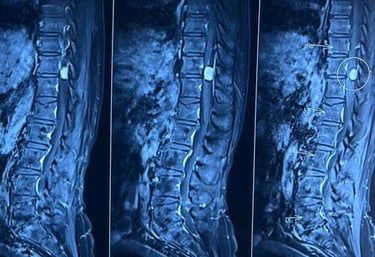
T1 CONTAST SAGITTAL
Heterogenously enhancing globular lesions forming acute angles with the dural margins. No dural tail, dorsal location and spanning typically a single or two vertebral levels, are features suggestive of a nerve sheath tumour.
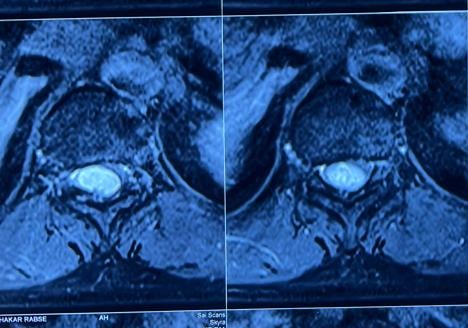
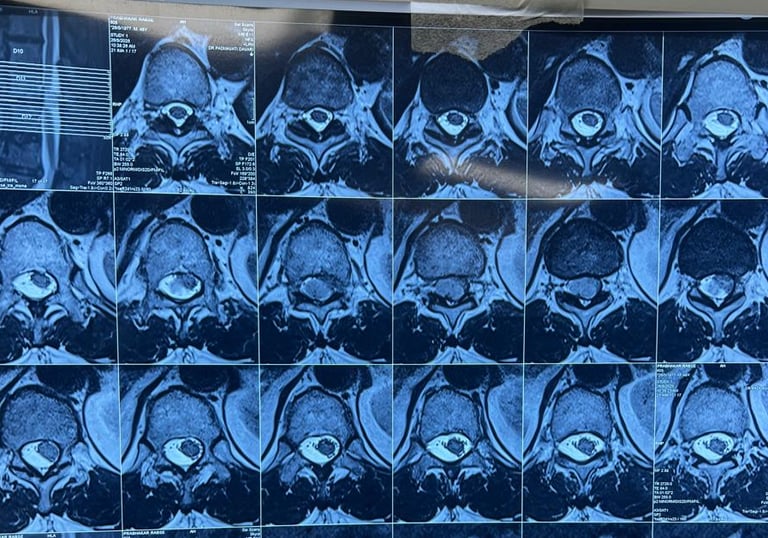
T1 CONTRAST AXIAL
Side and extent of spinal cord displacement is crucial in surgical planning. Small tumours involving less than half of the spinal canal may be approached via a hemilaminectomy.
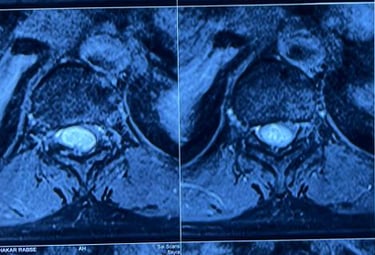
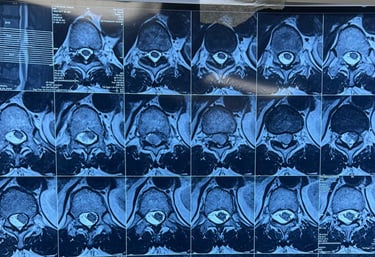
Typically T2 hyper intensity with a roundish appearance distinguish these tumours from meningiomas. As schwannomas commonly arise from dorsal rootlets, the spinal cord is almost always pushed anterolaterally, in contrast to meningiomas, where posterior cord displacement is not uncommon.
T2 W AXIAL
Patient Position & Exposure
Patient can be positioned on bolsters or a Wilson frame. Pressure points should be padded. Knees flexed. The abdomen and genitilia should be free.
PATIENT POSITION
The patient is positioned prone on bolsters with elbows and knees padded with the abdomen and genetilia free. Shoulders are abducted and moved out of the way for uninterrupted C arm views.


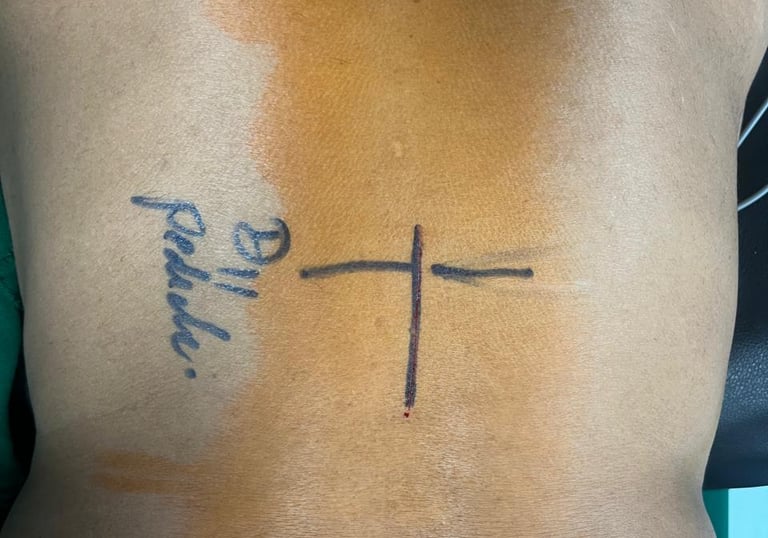
SKIN INCISION
A midline incision marked in the midline. Small tumours warrant small incisions and the use of Ramani retractors for 1 or 2 level laminectomies. Midline incisions and dissections especially in the dorsal spine, avoid blood loss and postoperative pain.
Subperiosteal dissection to expose the laminae overlying the tumour. Instead of aiming for the vertebral level, aim to remove precisely the bone overlying the tumour. In this case a 3/4 partial inferior D11 laminectomy and a 1/4th partial superior D12 laminectomy was performed.
INITIAL DISSECTION

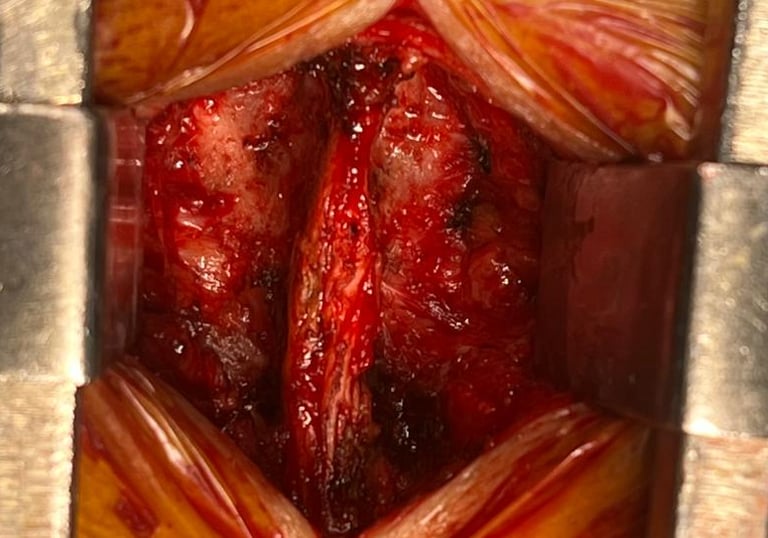
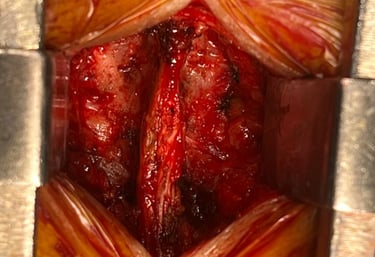
Surgical Nuances
With careful dissection and with the proper exposure, dorsal schwannomas practically deliver themselves. Adequate dural opening exposing both poles of the tumour, along with sharp arachnoid dissection away from the spinal cord are essential.
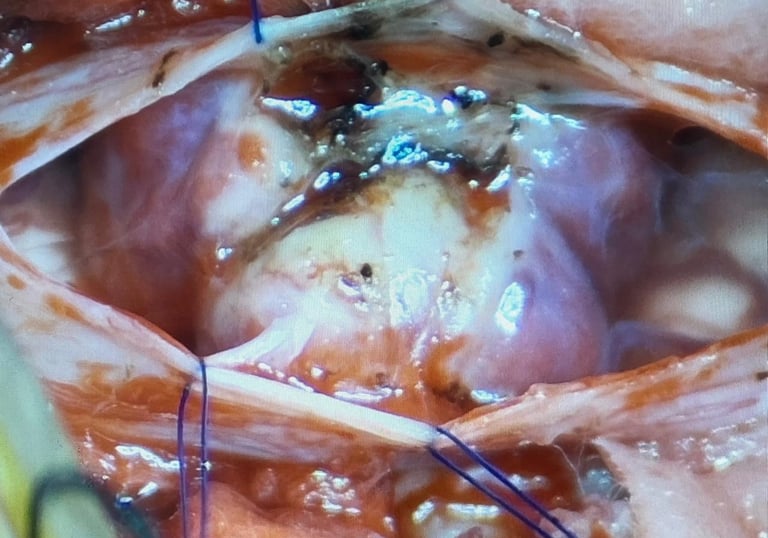
DURAL OPENING
After meticulous extradural hemostasis, the dura is opened in the midline. Arachnoid must be opened as a separate layer to prevent blood from entering the subarachnoid space. All layers of the dura must be opened together to minimise bleeding. Most of the dural bleeding stops when the dura is everted and tacking sutures are taken.


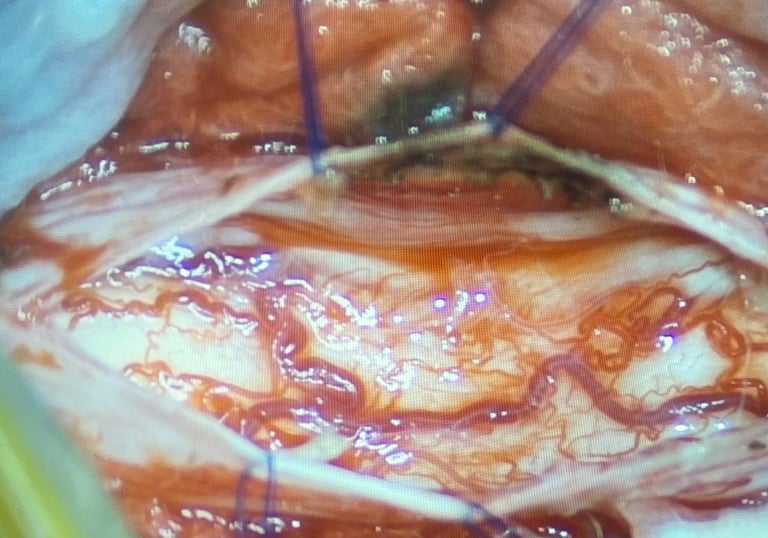
TUMOUR EXCISION
Both ends of the tumour should be well exposed to prevent blind dissection. Sharp arachnoid dissection, adequate debulking and maintaining the arachnoid plane of the tumour are crucial to prevent cord injury and preserve roots and bleed vessels.
MEP and SSEP monitoring can be used to ensure no functional damage. No vessel over the spinal cord surface must be coagulated. It is important to note the side and degree of displacement and compression of the cord and direct tumour dissection away from the side of the cord. 6 mg Dexamethasone, warm saline and maintaining a systolic BP of > 140 mmHg help in increasing cord perfusion and reducing neural injury and oedema due to handling.
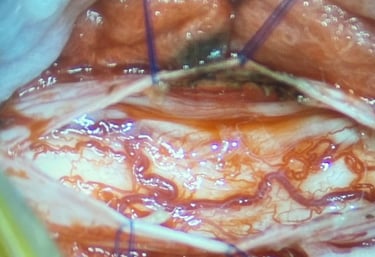
FUNCTIONAL PRESERVATION

Post op day 1
Patient mobilised with no neurological deficits.
Motor power 5/5 in all limbs
Sensations to fine touch, proprioception, temperature and pressure all normal over bilateral lower limbs and torso.
Discharged - Post op day 3
No neurological deficits.
Dorsal radiculopathy completely resolved.
(Picture published with permission)


Contact Us
We would love to hear from you!
For appointments kindly use the Consult portal.
Email: drmrudulbhatjiwale@gmail.com
Phone: +91-8421190149
© Mrudul Bhatjiwale 2025. All rights reserved.